- Description
- Software Downloads
- Documentation
- Screenshots & Examples
- Software Change Log
- FAQs
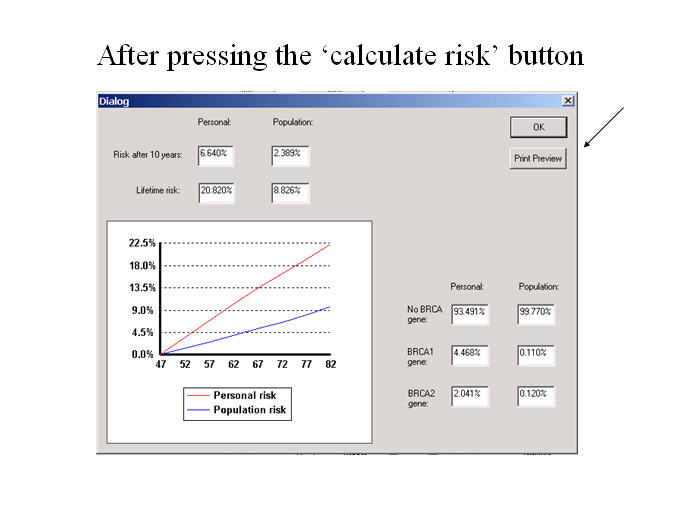
Description of breast cancer risk programThe program assumes that there is a gene predisposing to breast cancer in addition to the BRCA1/2 genes. The woman's family history is used to calculate the likelihood of her carrying an adverse gene, which in turn affects her likelihood of developing breast cancer. The risks of developing breast cancer for the general population were taken from data on the first breast cancer diagnosis (ICD-10 code C50) in Thames Cancer Registry area (UK) between 2005-2009.
The risk from family history (caused by the adverse genes) is modelled to fit the results in "Familial Breast and Ovarian Cancer: A Swedish Population-based Register Study, Anderson H et al., American Journal of Epidemiology 2000, 152: 1154-1163".
Contact DetailsProf. Sir Jack Cuzick PhD FRS CBE email: wiph-tyrercuzick@qmul.ac.uk |
Software
The current version of the software is v8. Versions 7 and 6 are obsolete but are available to download because they have been used in earlier research studies. Changes between versions are described in the change log. Please send any reports of bugs to wiph-tyrercuzick@qmul.ac.uk
Current version
| v8 (v8.0b latest release, September 2017) | |
| Windows download -- IBIS_RiskEvaluator_v8b.zip |
A beta batch web program is also available, for users who wish to process several risk evaluations at the same time for research without using a graphical user interface version. It requires uploading a text file input file to a website. Access it at tc-web-qkcz.onrender.com.
Obsolete versions
| v7 (version 7.02 released June 2013) | |
| Windows download -- IBIS_RiskEvaluator_v7.zip | |
| v6 (released August 2004) | |
| Windows download -- IBIS Risk Evaluator.zip | |
| Example.txt |
Overview of evaluator
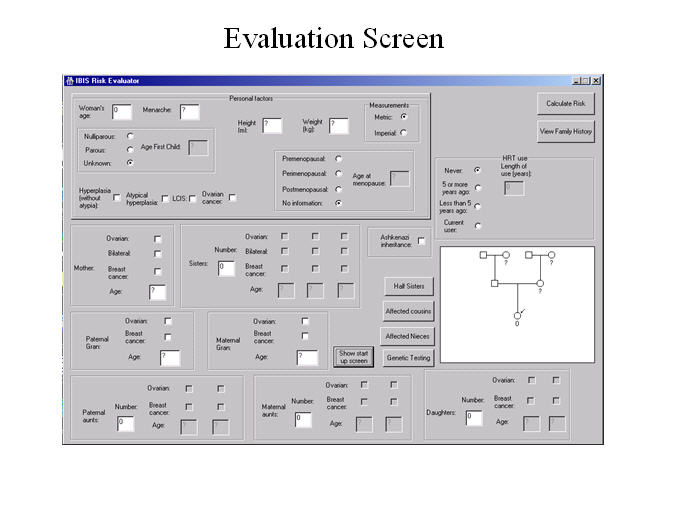
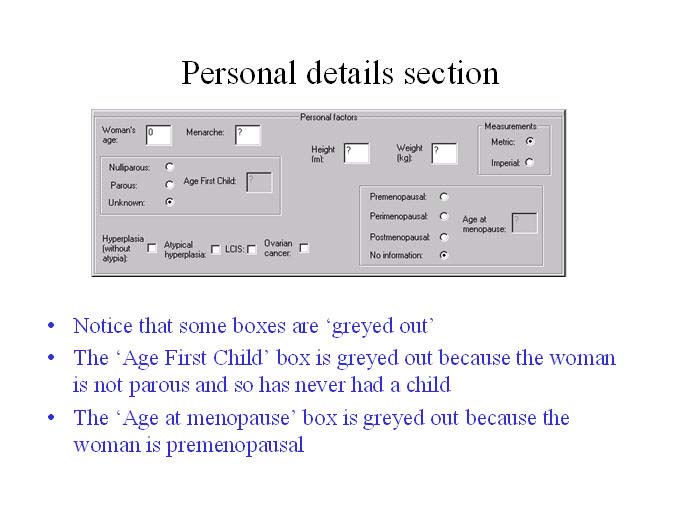
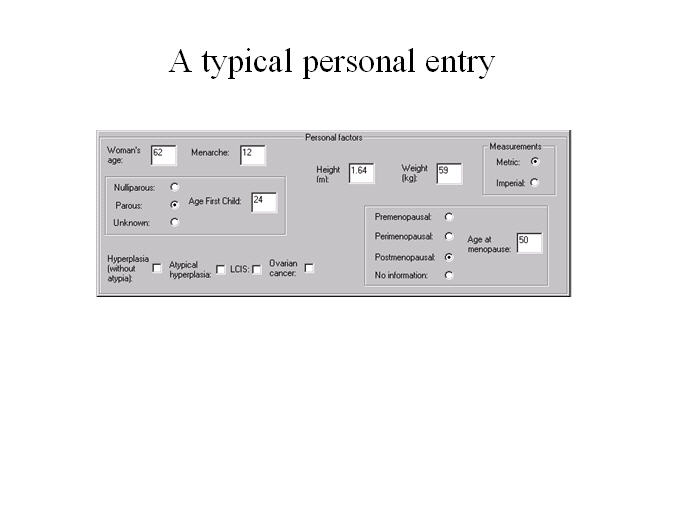
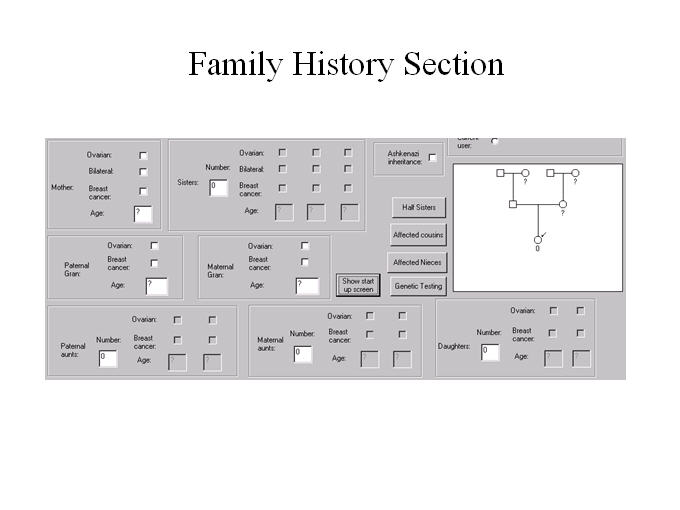
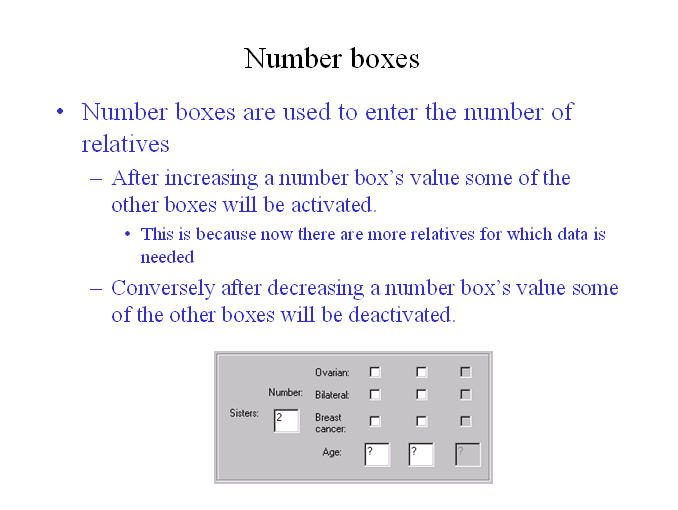
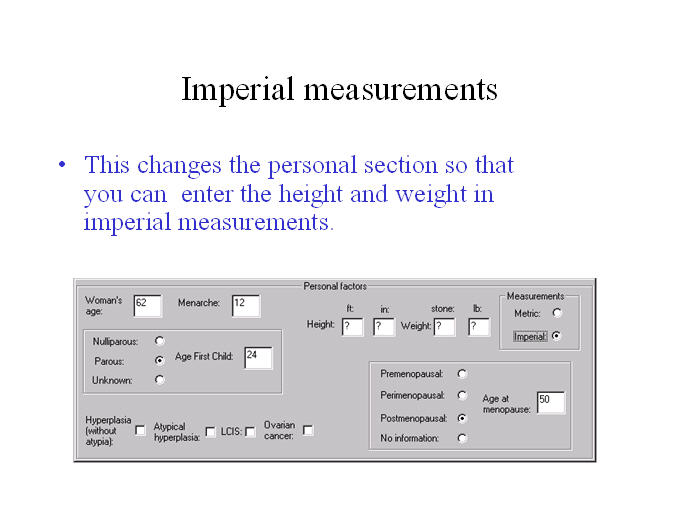
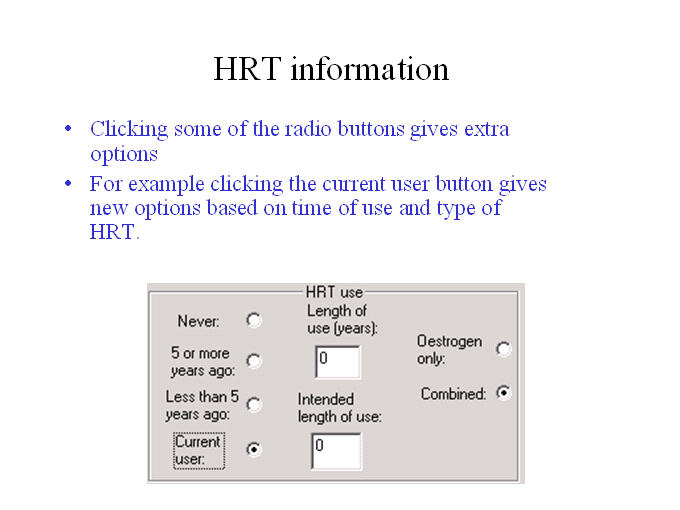
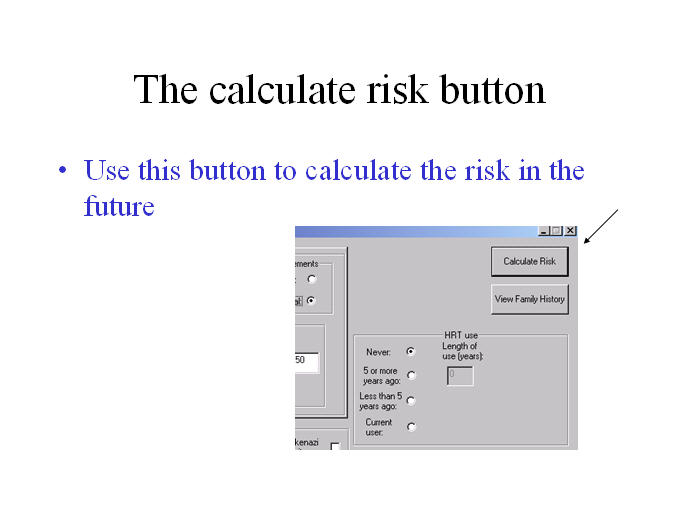
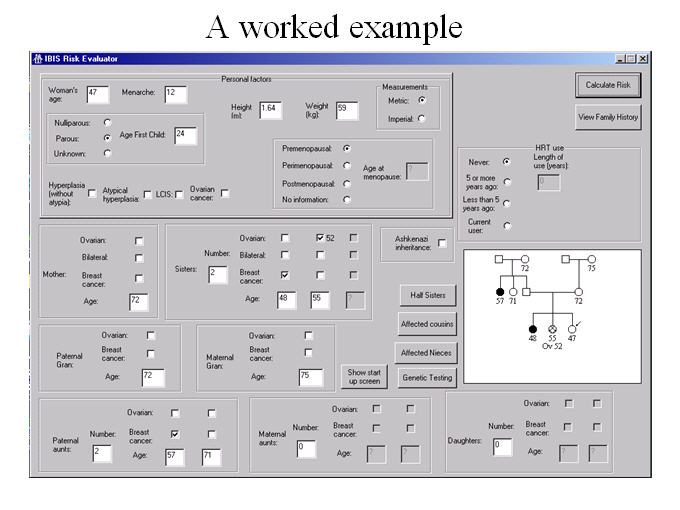
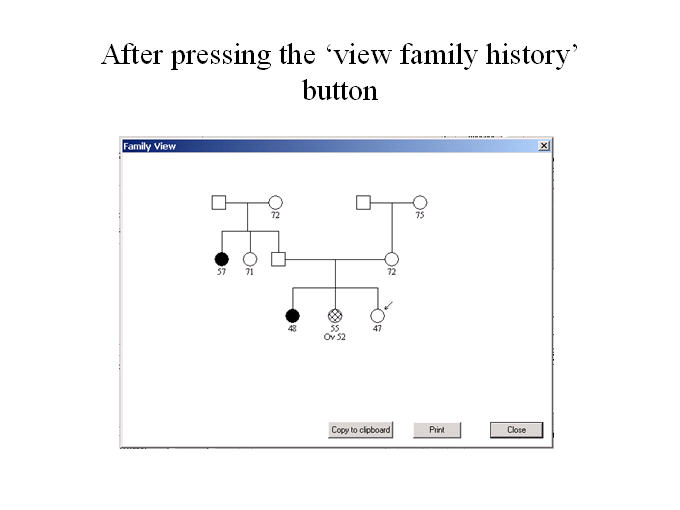
The program begins by opening the introduction screen. If you want to go directly to the evaluation screen the next time the program is run then you should tick the ‘Start from evaluation screen’ box. The top part of the evaluation screen deals with personal information about the woman - her age at menarche, parity etc. The bottom part of the screen deals with her family history. The picture in the form gives the family history in the form of a pedigree diagram. When entering details about a family member, if she developed breast cancer then the age at breast cancer should be put in the relevant age box, otherwise her current age should be used (or the age at which she died if applicable). If she developed ovarian cancer then a box is activated which asks for details at which age it occurred. Similarly if she developed bilateral breast cancer then a box is activated which asks for the age at which breast cancer developed in the second breast. If age is not known then ‘?’ should be entered in the age box. If it is not known whether a relative developed breast cancer then ‘u’ should be typed in the age box to represent no information. If the woman has an affected niece in the family then the affected niece button should be pressed to enter the details. The tools menu gives you options to choose the number of years to risk, whether to allow for competing mortality risks, and to choose population rates (UK, Sweden or Slovenia). v8: Information on mammographic density is given in the model under the Help menu. If entering mammographic density, then it is also very important to enter height and weight to obtain the most accurate risk assessment for an individual woman. More documentation may be downloaded from the following links.
For further information on mammographic density please follow the following links.
*BI-RADS® ATLAS is a registered trademark of American College of Radiology. All rights reserved. The developer of this product is independently owned and operated, and is not an affiliate of the American College of Radiology. The American College of Radiology is not responsible for the contents or operation of this product or its associated software, and expressly disclaims any and all warranties and liabilities, expressed or implied, in connection therewith. |
Please click on an image below from an enlarged view
| All images can be found in a powerpoint presentation that is available for download |
||
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
||
Summary of version changes
Changes to version 8Main changes
Minor changes
Bug fixes
Beta version changes
Changes to version 7Main changes
Some more minor changes have also been made.
Version 7 bug fixes and updates
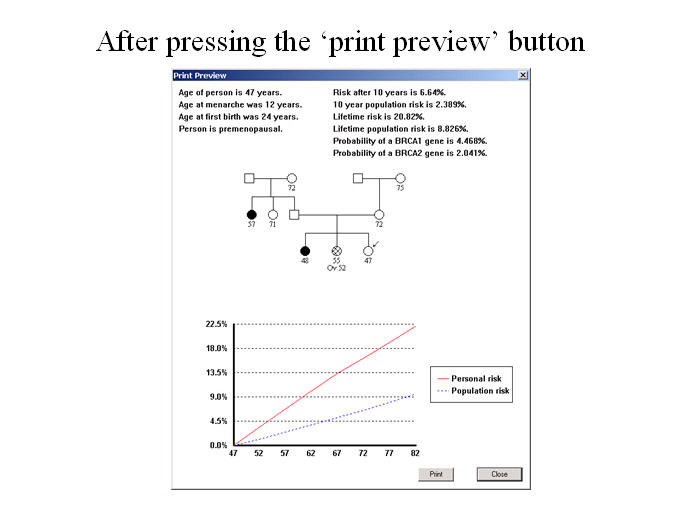
Changes to version 6The program now allows you to save patients’ details. Also more information about the woman is given in the print preview screen. A number of other options are available in the toolbar. These are Add – Add a patient to the file. Format of text file used for saving patients’ details (only needs to be known if using the program for batch input)Version number (in this case “v6”) Changes to version 5.1Added “Copy to Clipboard” option for print preview screen so that user can paste results into Word or PowerPoint. Changes to version 5
|
FAQs
-
v8 and v7 give higher lifetime risks than v6. Why?
 Figure 1. UK Breast cancer incidence (C50, invasive) in 1994 and 2008-2010 (source: Cancer Research UK).
Figure 1. UK Breast cancer incidence (C50, invasive) in 1994 and 2008-2010 (source: Cancer Research UK).Table 1 Breast cancer rates (per year, 100K) used in the models. Age group v6 v7/8 (UK) v7/8 (Sweden) 20 – 24 1.2 1.3 1.0 25 – 29 8.0 9.1 7.0 30 – 34 26.6 24.2 24.6 35 – 39 60.7 57.5 50.2 40 – 44 112.6 115.6 108.4 45 – 49 180.3 182.3 188.5 50 – 54 244.2 250.3 217.9 55 – 59 256.5 266.2 248.9 60 – 64 277.1 318.7 324.8 65 – 69 244.3 378.5 363.4 70 – 74 283.1 296.4 336.9 75 – 79 328.7 331.9 274.3 80 – 84 357.2 369.7 307.6 There are two main reasons. Firstly, lifetime risk from v7+ runs to age 85; in v6 it was until age 80. Secondly, the population rates used have been updated to be more applicable for risk assessment of women today. Figure 1 shows how incidence has risen between 1994 and 2008-2010; Table 1 summarises the difference between the rates used by versions 6-8. The main difference is that in 1994 women in the UK were not screened beyond age 64 (V6). The increase in rates beyond 60 mostly reflects more screening in these age groups between 2005-2010 than in 1994. Differences between UK (Thames Registry first breast cancer rates 2005-2009) and Sweden (Statistics Sweden first breast cancer rates 2006-2010) might also be explained by temporal differences in screening regimens, including that Sweden has screened later ages for longer than the UK.
-
v8 identifies more women at high risk than v7. Why?
The main reason is that it includes more risk factors (density and SNPs). Both of these with increase the number of women accurately identified to be at high risk. If they are incorporated into the risk assessment then more women will be at high (and low) risk than when they are not used.
-
Are the rates used appropriate for the USA, or other countries?
The model uses a `period' epidemiological approach, and is calibrated to first breast cancer diagnosis rather than incidence. First breast cancer rates are not usually published. However, one way to assess whether the model is broadly in alignment is to use the SEER age-standardised incidence. Over the period 2005-2009 in the Thames cancer registry this was 119.5, and may be directly compared with the numbers published by the NCI on their website (last accessed 14th June 2013). For example, the SEER age-standardised rate between 2005-2009 in Georgia was 119.7. For comparison, the SEER age-standardised UK first cancer rate that is used in V7 is 114.7.
-
Why is competing mortality not default?
Lifetime risk including the competing mortality option gives an assessment that allows from death from other causes than breast cancer. It is not used by default for consistency: cumulative incidence is usually presented conditional on no intercurrent mortality. However, it is easy to toggle back and forth on the form by using the checkbox next to the risk assessment button.
-
What are the benign breast biopsy categories?
Table 2 Breast biopsy risk classification to use in model. Adapted from Page and Dupont (1993), http://dx.doi.org/10.1007/bf00666428. No benign disease (includes no proliferative disease) Adenosis Apocrine change Duct ectasia Mild epithelial hyperplasia of usual type Hyperplasia (not atypia) (Proliferative disease without atypia) Hyperplasia of usual type, moderate or florid Papilloma (probably) Sclerosing adenosis Atypical hyperplasia Atypical ductal hyperplasia Atypical lobular hyperplasia LCIS Lobular carcinoma in situ The benign disease categorisation shown in Table 2 is based on the classical work from Page and Dupont (1993, link); see also Hartmann et al (2005, link). Fibroadenomas are considered nonproliferative unless they also contain a proliferative lesion. The 'unknown' category is for when the result from a prior biopsy is unknown.
-
Have there been any publications validating the model for risk evaluation?
Work is ongoing in a number of studies. Some articles to specifically address this issue include the following.
- Cuzick, J., Brentnall, A. R., Segal, C., Byers, H., Reuter, C., Detre, S., Lopez-Knowles, E., Sestak, I., Howell, A., Powles, T. J., Newman, W. G., Dowsett, M. To appear 2017. Impact of a panel of 88 single nucleotide polymorphisms on the risk of breast cancer in High-Risk women: Results from two randomized tamoxifen prevention trials. Journal of Clinical Oncology. URL
- Evans, D. G., Brentnall, A., Byers, H., Harkness, E., Stavrinos, P., Howell, A., risk study Group, F., Newman, W. G., Cuzick, J., Oct. 2016. The impact of a panel of 18 SNPs on breast cancer risk in women attending a UK familial screening clinic: a case–control study. Journal of Medical Genetics. URL
- Brentnall, A. R., Harkness, E. F., Astley, S. M., Donnelly, L. S., Stavrinos, P., Sampson, S., Fox, L., Sergeant, J. C., Harvie, M. N., Wilson, M., Beetles, U., Gadde, S., Lim, Y., Jain, A., Bundred, S., Barr, N., Reece, V., Howell, A., Cuzick, J., Evans, D. G., Dec. 2015. Mammographic density adds accuracy to both the Tyrer-Cuzick and gail breast cancer risk models in a prospective UK screening cohort. Breast Cancer Research 17 (1), 147+. URL
- Warwick, J., Birke, H., Stone, J., Warren, R. M. L., Pinney, E., Brentnall, A. R., Duffy, S. W., Howell, A., Cuzick, J., Oct. 2014. Mammographic breast density refines Tyrer-Cuzick estimates of breast cancer risk in high-risk women: findings from the placebo arm of the international breast cancer intervention study i. Breast Cancer Research 16 (5), 451+. URL
- Quante, A. S., A. S. Whittemore, T. Shriver, K. Strauch, and M. B. Terry (2012). Breast cancer risk assessment across the risk continuum: genetic and nongenetic risk factors contributing to differential model performance. Breast cancer research : BCR 14 (6), R144+.
- Amir, E., D. G. Evans, A. Shenton, F. Lalloo, A. Moran, C. Boggis, M. Wilson, and A. Howell (2003). Evaluation of breast cancer risk assessment packages in the family history evaluation and screening programme. Journal of medical genetics 40 (11), 807-814.